Pregnant patients with RA require team work between their rheumatologist and obtetrician.
 1. Plan for pregnancy and discuss the issues well ahead of time: It is best to anticipate what will need to be done.
1. Plan for pregnancy and discuss the issues well ahead of time: It is best to anticipate what will need to be done.
2. Have a plan as to how to use medications.
Some effective RA drugs are considered safe for use during pregnancy. Some patients opt to discontinue all RA drugs during pregnancy rather than take any risks. The problem with this approach is that a flare up of RA which can affect the outcome for mother and child.
No drug used in RA is licenced to be used in pregnancy. However, prednisone, hydroxychloroquine, and TNF inhibitors are now regarded as safe during pregnancy;
methotrexate and leflunomide are not.
Nonsteroidal anti-inflammatory drugs (NSAIDs) slightly inhibit fertility in the preconception period.
While NSAIDs are safe during the first and second trimesters, they have to be stopped during the third, when they can cross the placenta and interfere with the fetal heart and lungs.
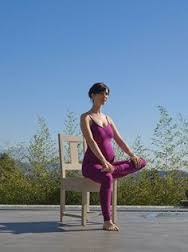 3. Keep fit during the pregnancy and maintain hip flexibility and shoulder and arm and hand strength.
3. Keep fit during the pregnancy and maintain hip flexibility and shoulder and arm and hand strength.
4. Breast feeding.
Any women who chooses to breastfeed can be assured that the medications that are safe during pregnancy are also safe during lactation.
5. A postpartum flare is possible
The postpartum disease flare is a well-known phenomenon in RA and is best planned for before delivery.
Identify and have a plan to manage any physical disability that may impact on caring for the baby.
In January 2016 further information became available.
Bristish Society of Rheumatology releases guidelines for DMARD use during pregnancy
January 15, 2016
“The management of patients with inflammatory rheumatic diseases during pregnancy is complicated by several factors, including an increased burden of pregnancy morbidity that is partly due to increased disease activity, and so it is vital to maintain adequate control of disease activity with medications that are compatible with pregnancy,” according to a press release from the society.
Among the highlights of the guidelines, the British Society for Rheumatology (BSR) recommends:
· prednisolone as the corticosteroid of choice, which the group said is compatible during all trimesters;
. use of hydroxychloroquine as an antimalarial prior to conception and throughout pregnancy;
· discontinuation of methotrexate 3 months prior to conception and avoidance of this medication during the entire pregnancy;
. avoidance of adalimumab and etanercept in the third trimester, and discontinuation of infliximab at 16 weeks of pregnancy. If these treatments are used later in pregnancy, live vaccinations should be avoided for the infant through age 7 months;
. certolizumab pegol as a treatment based on limited evidence that it is compatible in all trimesters of pregnancy.
“The BSR guidelines will enable medical practitioners to have a more confident and consistent approach to prescribing anti-rheumatic drugs in pregnancy and breastfeeding,” Ian Giles, PhD, FRCP, professor at the Centre for Rheumatology Research at the University College London Division of Medicine, said in the release. “I hope this approach will allow adequate control of inflammatory rheumatic disease activity and prevent the unnecessary withdrawal of disease ameliorating anti-rheumatic therapies which have not been shown to be harmful in pregnancy and breastfeeding.”
Reference:
www.rheumatology.org.uk
References:



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}